Trigeminal neuralgia, often called “tic-douloureux,” is a chronic pain disorder that affects the trigeminal (cranial nerve V) sensory pathway. It is characterized by sudden, severe, electric-shock-like facial pain that can be triggered by everyday activities such as chewing, speaking, brushing teeth, or even a light breeze.
What is Trigeminal Neuralgia?
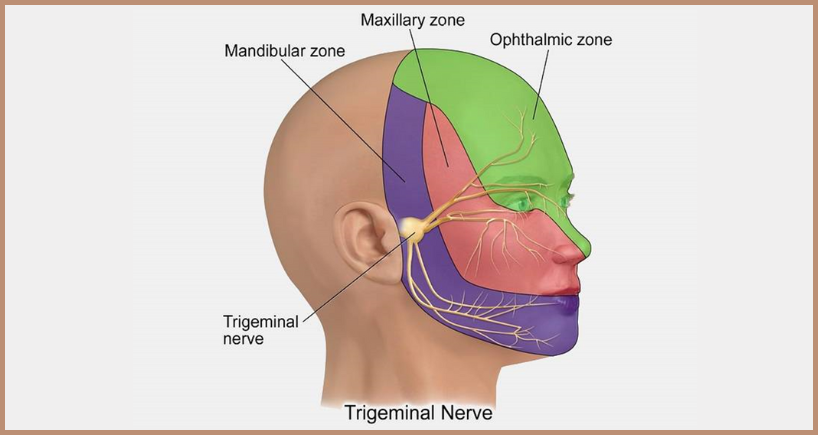
Definition: A neuropathic pain condition caused by irritation or compression of the trigeminal nerve’s root entry zone, most commonly by an adjacent blood vessel.
• Epidemiology: Typically presents after age 50; women are affected slightly more often than men. Incidence is about 12–13 per 100,000 people per year.
• Types:
o Classical (idiopathic) – vascular compression without other pathology.
o Secondary (symptomatic) – associated with multiple sclerosis plaques, tumors, or
skull base lesions.
Typical Clinical Presentation
Pathophysiology
• Neurovascular compression: A looping artery or vein exerts pulsatile pressure on the nerve, leading to demyelination and ectopic impulse generation.
• Demyelination: Loss of myelin sheath causes cross-talk between fibers, resulting in hyperexcitability.
• Secondary causes: Demyelinating diseases (e.g., multiple sclerosis), space-occupying lesions, or post-traumatic scarring.
Diagnostic Approach
- Detailed history – Focus on pain characteristics, triggers, and distribution.
- Neurological exam – Usually normal between attacks; check for sensory deficits.
- Imaging – High‑resolution MRI with FIESTA or CISS sequences to visualize neurovascular conflict and rule out secondary causes.
- Diagnostic criteria (ICHD‑3) – Must meet specific pain pattern, trigger zones, and exclusion of other disorders.
Management Strategies
- Pharmacologic First-Line
- Carbamazepine – 100–1200 mg/day divided doses; monitor serum levels and side-effects (dizziness, hyponatremia).
- Oxcarbazepine – Similar efficacy, better tolerability for some patients. Trigeminal Neuralgia
- Adjuncts – Baclofen, lamotrigine, gabapentin, or pregabalin for refractory cases.
- Interventional Options (when meds fail or cause intolerable side-effects)
- Microvascular Decompression (MVD) – Surgical relocation of offending vessel; offers long-term relief in >70% of patients.
- Percutaneous Procedures – Radiofrequency rhizotomy, glycerol injection, balloon compression; provide rapid pain control but may need repeat.
- Stereotactic Radiosurgery (Gamma Knife) – Non-invasive; pain relief often delayed (weeks-months) with variable durability.
- Supportive Care
- Patient education – Explain triggers, medication adherence, and potential side-effects.
- Psychological support – Chronic facial pain can cause anxiety and depression; consider counseling or support groups.
- Dental coordination – Inform dentists to avoid unnecessary procedures that may trigger pain.
- Classical TN: Many achieve long‑term remission after successful MVD; pharmacologic controlis often adequate for years.
- Secondary TN: Prognosis depends on underlying disease; MS‑related TN may respond less predictably to surgery.
Frequently Asked Questions (FAQs)
A neuropathic facial pain disorder caused by irritation or compression of the trigeminal nerve (cranial nerve V). Pain is sudden, electric-shock-like, and triggered by light stimuli.
No. Patients often have pain‑free intervals lasting days, weeks, or months.
• Detailed history and neurological exam.
• High‑resolution MRI (FIESTA/CISS) to identify neurovascular compression and rule out secondary causes (tumor, MS).
Not “cured” in the classic sense, but many patients achieve long‑term pain control with medication or surgery. Success rates: MVD > 70% sustained relief; percutaneous procedures 50‑80% short‑term relief.
Untreated TN can lead to anxiety, depression, and social isolation. Effective treatment dramatically improves daily functioning and mood.



